


1/1/2026
5 Signs Your Benefits Portfolio Has a Comorbidity Gap
Most benefits portfolios were not designed. They were assembled. One vendor for diabetes. Another for MSK. A third for behavioral health. A fourth for weight management, usually filed under wellness. Each solution added in response to a trend report or a renewal conversation, rarely in conversation with the others.
The result is a portfolio that looks comprehensive on a benefits guide and functions as a collection of disconnected programs when a member actually needs care. The clinical problem with that architecture is comorbidity. The financial problem is that comorbidity is where your highest-cost members live.
Among adults with a chronic condition, more than 60% carry at least one additional diagnosis. A portfolio built condition by condition cannot manage members whose conditions interact. Here are five signals that your benefits portfolio has a comorbidity gap, and that it is costing you more than you can see in any single vendor's report.
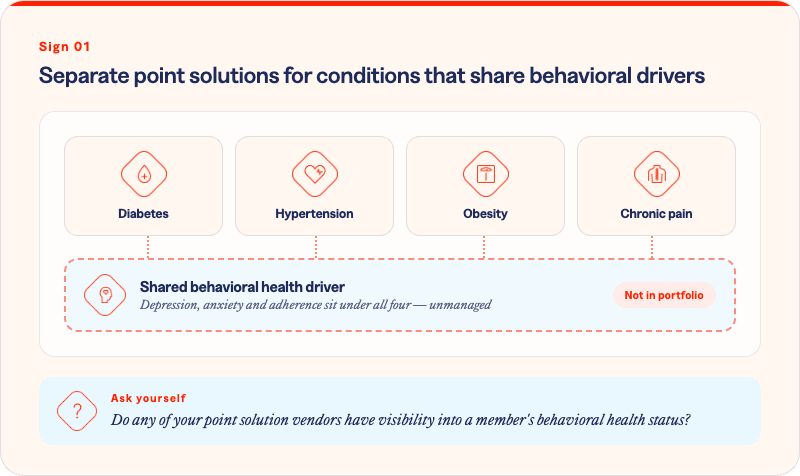
Diabetes. Hypertension. Obesity. Chronic pain. Each of these conditions has a strong behavioral health dimension: depression and anxiety are both risk factors and consequences, medication adherence is behaviorally driven, and lifestyle modification depends on mental health stability as much as clinical instruction.
If your benefits portfolio routes each of these conditions to a separate program with no shared behavioral health layer, you are treating the clinical presentation and ignoring the behavioral driver. A member managing type 2 diabetes with untreated depression will underperform on every clinical metric that program tracks, and that underperformance will be invisible to the diabetes vendor.
Point solutions are designed to optimize within a condition. They are structurally incapable of seeing, or addressing, what is happening across conditions.

This is the most common and most costly structural gap in a siloed benefits architecture. If your quarterly reviews consist of separate reports from each vendor showing engagement rates, satisfaction scores, and within-program outcomes, you do not have a population health picture. You have a collection of vendor performance stories.
The members generating your highest claims are almost never high-cost within a single condition. They are high-cost across several. A member with co-occurring diabetes, MSK, and behavioral health diagnoses will appear as a moderate-cost member in three separate reports. In your claims data, they are one of your most expensive members.
Cross-condition reporting is not a reporting preference. It is the only way to see the population you are actually managing. Without it, your interventions are optimized for conditions that do not exist in isolation in your highest-risk members.
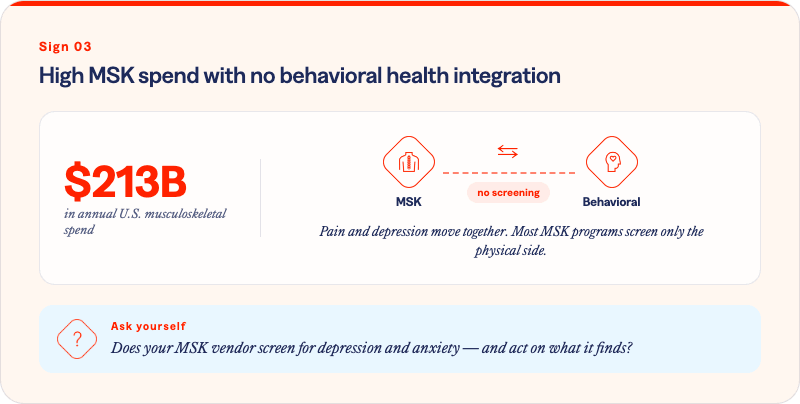
Musculoskeletal disorders account for more than $213 billion in annual U.S. healthcare expenditure. If MSK is a top cost driver in your population and your MSK program has no behavioral health component, you are missing a primary driver of both outcomes and spend.
Chronic pain and behavioral health have a well-documented bidirectional relationship. Depression lowers pain tolerance, reduces physical activity, and impairs rehabilitation engagement. Members managing chronic MSK conditions alongside untreated depression or anxiety have longer recovery timelines, higher surgical rates, and significantly higher total cost of care.
The same relationship holds for surgery avoidance. A member who completes a digital MSK program but is managing untreated anxiety is less likely to adhere, less likely to achieve functional improvement, and more likely to end up in the surgical pathway that the program was designed to prevent.

Type 2 diabetes and hypertension co-occur at high rates. The upstream metabolic risk factors are largely shared. The medication regimens interact. The lifestyle interventions overlap significantly. And yet the majority of benefits portfolios route these conditions to separate point solutions that do not communicate.
The clinical consequence is care that is fragmented at exactly the level where coordination would produce the most value. A member receiving diabetes coaching from one vendor and hypertension management from another is navigating two separate engagement experiences, two separate care plans, and two separate check-in cadences, none of which account for the other.
Add the behavioral health dimension that frequently underlies both conditions, and the coordination failure is compounded. The member is not receiving integrated care. They are receiving three siloed programs that each count them as an enrolled participant.
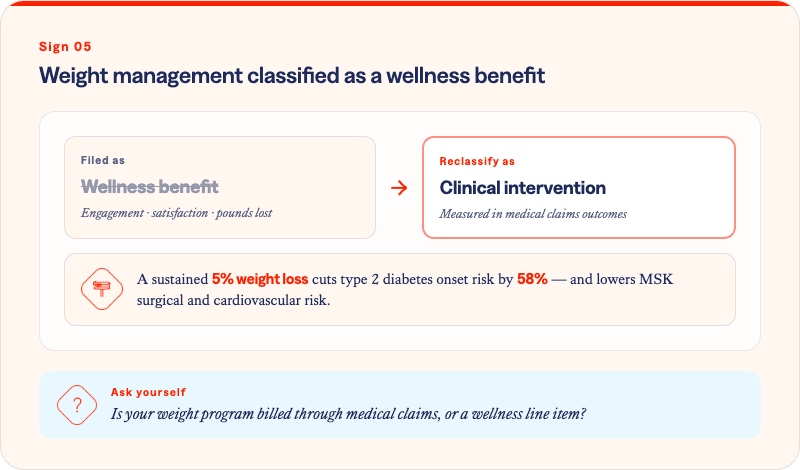
This is the most consequential categorization error in most employer benefits portfolios. Weight management drives downstream cost across your most expensive condition categories: type 2 diabetes, MSK disorders, cardiovascular disease, hypertension, and behavioral health. When it is classified as a wellness benefit, it is evaluated on wellness metrics: engagement rates, satisfaction scores, pounds lost.
None of those metrics connect to claims. None of them answer the CFO's question. And none of them reflect what a clinically meaningful weight loss outcome, defined as a sustained 5% reduction in body weight, actually produces: a 58% reduction in T2D onset risk, measurably reduced MSK surgical risk, and lower cardiovascular event rates.
When weight management is a wellness benefit, it competes with gym subsidies for budget. When it is reclassified as a clinical intervention with claims-based outcome measurement, it becomes one of the highest-leverage investments in your portfolio.
The comorbidity gap is not a clinical problem. It is an architecture problem.
Siloed benefits portfolios were designed to manage individual conditions at scale. They were not designed to manage the 60% of members who carry more than one. Closing the comorbidity gap means moving from a vendor roster to an integrated population management model, one that can see the clusters, intercept them early, and measure what changes when it does.
See what integrated condition management looks like across your population.
Solera Health's network addresses comorbidity at the population level, connecting members to evidence-based digital health programs across condition areas, matched by clinical profile and measured through medical claims outcomes.
Explore Other Resources
6/1/2026

The Network Effect: Proving the Value of Curated Digital Health
$1,241 — Total cost of care reduction per member
5/15/2026
Employer Health Care Costs in 2026: What’s Driving the Spike and What’s Actually Working
Do Digital Health Programs Reduce Employer Health Care Costs?
4/6/2026
Death By a Thousand Vendors: A Study of 106 Senior Benefits Leaders
More vendors. More spend. More headcount. And yet — the problem is getting worse.
.png)