


1/1/2026
DPP vs. IBT vs. Clinical: How to Choose the Right Weight Management Intervention for Your Population
Not every member with excess weight needs the same intervention. A prediabetic member at 28 BMI and a member with severe obesity and three comorbidities are not the same clinical profile, and routing them to the same program is a benefits design failure, not a cost-neutral default.
Most employer weight management benefits offer one program type and call it coverage. The result is a population where the highest-risk members are enrolled in programs not designed for their clinical complexity, lower-risk members who could achieve meaningful outcomes with lighter-touch support are over-resourced, and the claims impact of the entire investment is diluted by poor matching.
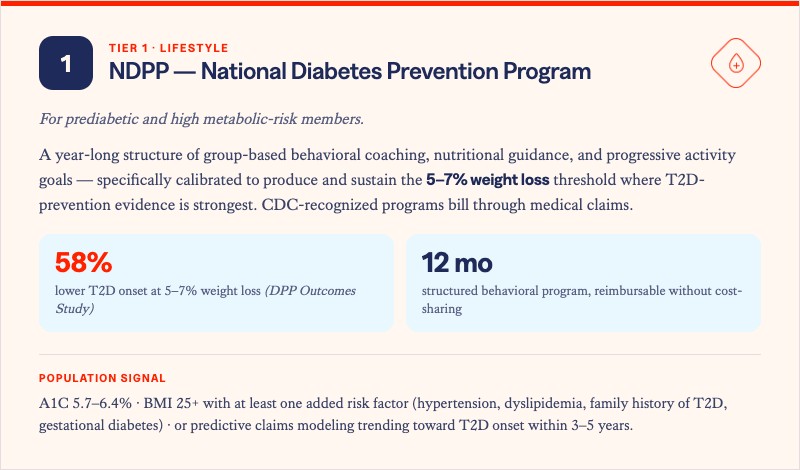
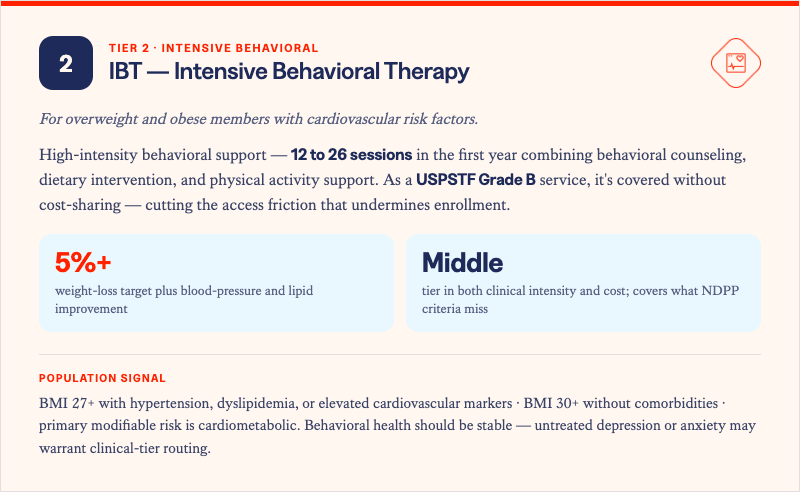
The evidence base for weight management is program-type specific. The National Diabetes Prevention Program works for the prediabetic population because it was designed and validated for that population. Intensive Behavioral Therapy works for members with cardiovascular risk factors because it meets the USPSTF evidentiary standard for that cohort. Clinical and virtual clinic programs exist because neither of the above is designed for members with severe obesity and complex medical needs.
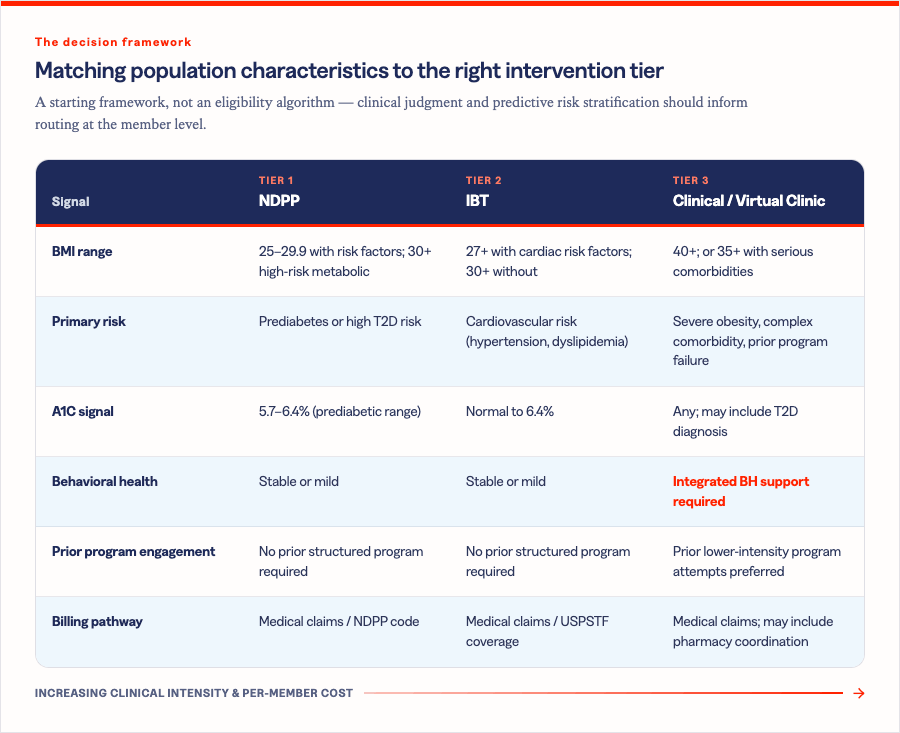
Here is a practical frameworkfor how benefits leaders and consultants should think about population segmentation and program matching across the three major intervention tiers.

The decision framework
The table below maps population characteristics to the appropriate intervention tier. It is a starting framework, not an eligibility algorithm -- clinical judgment and predictive risk stratification should inform routing decisions at the member level.
What integrated tier management looks like in practice
A benefits architecture that supports all three tiers does not mean three separate vendor contracts with no coordination. It means a single population identification and routing infrastructure that can match members to the appropriate program level based on clinical profile, risk stratification, and prior engagement history, and that tracks outcomes across tiers as members' needs evolve.
Solera can help to identify members across the weight management risk spectrum before high-cost events occur. The HALO Platform routes those members to matched programs within the network, spanning NDPP, IBT,and clinical tiers, with outcomes tracked through medical claims. When a member's clinical profile changes, their program routing can change with it -- without requiring a new benefits RFP or a new vendor relationship.
The goal is not to offer three programs. It is to have the right member in the right program at the right moment, with a measurement framework that documents what changes when they are.
Population-level weight management ROI depends on matching. A single-program benefits design is leaving a significant share of your highest-risk members unserved.
Solera Health connects benefits leaders and health plan executives to evidence-based digital weight management programs across the full intervention spectrum, matched to member risk profiles through predictive claims modeling and measured through medical claims outcomes.
Explore Other Resources
6/1/2026

The Network Effect: Proving the Value of Curated Digital Health
$1,241 — Total cost of care reduction per member
5/15/2026
Employer Health Care Costs in 2026: What’s Driving the Spike and What’s Actually Working
Do Digital Health Programs Reduce Employer Health Care Costs?
4/6/2026
Death By a Thousand Vendors: A Study of 106 Senior Benefits Leaders
More vendors. More spend. More headcount. And yet — the problem is getting worse.
.png)