


1/1/2026
EAP vs. Digital Behavioral Health: Why the Comparison Misses the Point
EAPs do what they were designed to do. The problem is that what they were designed to do and what your population actually needs are not the same thing, and treating them as equivalent is producing a behavioral health strategy that serves a fraction of the members who need it.
The EAP versus digital behavioral health conversation usually gets framed as a cost comparison or a channel preference. That framing misses the structural point. EAPs and digital behavioral health programs are not different delivery mechanisms for the same intervention. They are designed for different populations, different acuity levels, and different clinical purposes. Running them as competitors in a benefits evaluation is like evaluating urgent care and primary care as alternatives rather than complements.
Understanding the distinction is not academic. It determines whether your behavioral health benefits actually reach the members generating the highest clinical and financial burden in your population.
What EAPs were designed for and where they deliver well
Employee assistance programs were built for acute situational crises: bereavement, workplace conflict, relationship distress, financial stress, and brief episodes of anxiety or depression triggered by identifiable life events. They are short-term, problem-focused, and designed to connect a member in acute need to a counselor quickly, typically within 24 to 48 hours.
For that use case, EAPs function as intended. A member navigating a sudden personal crisis does not need a six-month CBT protocol. They need immediate access to a trained counselor who can provide short-term support and, where needed, refer to longer-term care. EAPs fill that role and should remain part of a complete benefits architecture.
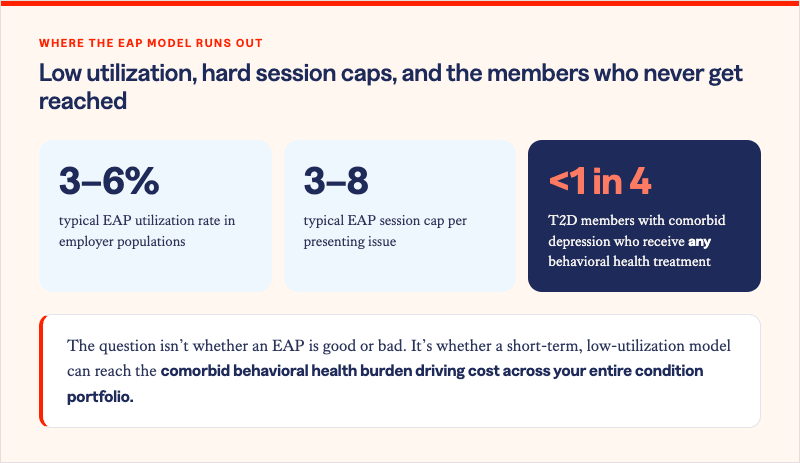
The structural problem arises when an EAP is positioned, either by design or by default, as the behavioral health benefit for a population that includes members with chronic depression, anxiety disorders, and the behavioral health comorbidities that co-occur with diabetes, MSK conditions, and cardiovascular disease. That is not the population EAPs were built to serve. And the data shows it.
The four structural gaps that limit EAPs at the population level
Low utilization rates. EAP utilization in employer populations consistently runs between 3 and 6%. That figure is not a marketing problem or an awareness problem. It is a design outcome. Members with the most significant and sustained behavioral health burden, those managing chronic depression alongside T2D or chronic pain, are precisely the members least likely to self-navigate to a short-term, stigma-adjacent resource. The members who most need behavioral health support are the ones least likely to call an EAP.
Short-term session caps. Most EAP contracts provide three to eight sessions per presenting issue. For a member managing acute situational distress, that is often sufficient. For a member whose depression is neurologically driven, metabolically reinforced by insulin resistance, and behaviorally entrenched across years of chronic disease management, it is not. Session caps do not match clinical need. They match administrative convenience.
No acuity matching. EAP intake processes are not designed to stratify members by clinical severity or match them to the appropriate level of care. A member presenting with mild situational anxiety and a member presenting with moderate recurrent depression who also has uncontrolled T2D are routed to the same resource. Acuity-appropriate matching, the mechanism by which high-risk members get higher-intensity support, does not exist in the EAP model.
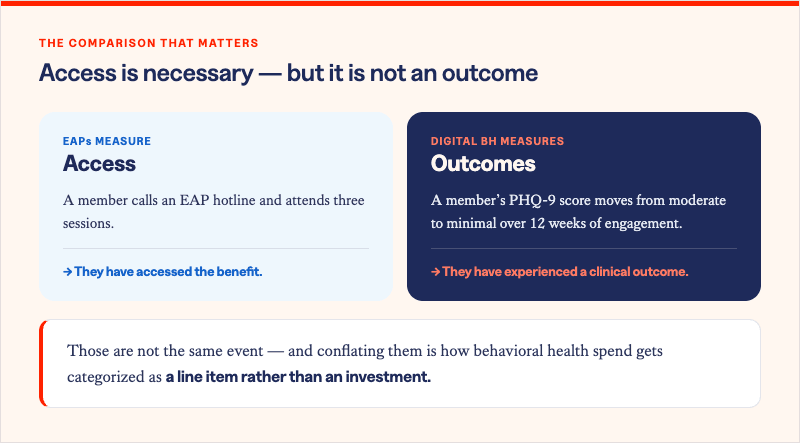
No clinical outcomes tracking. The standard EAP reporting package includes utilization counts, presenting issues by category, and average sessions per case. What it does not include is PHQ-9 scores at intake and discharge, GAD-7 trajectory over a member's engagement period, or any connection between behavioral health program participation and chronic condition outcomes. The absence of clinical outcome measurement is not a reporting gap. It is a design signal about what the program was built to optimize.
What digital behavioral health programs are designed to do differently
Digital behavioral health programs are not simply EAPs delivered through an app. They are clinically structured programs built for population-level deployment, acuity stratification, and longitudinal outcome measurement.
Broader reach through lower friction. Digital programs reach members who would not call an EAP: those who experience stigma around seeking mental health support, those whose behavioral health needs are subclinical but clinically significant, and those managing chronic conditions where behavioral health is a comorbidity rather than a presenting crisis. Asynchronous access, text-based options, and self-directed entry points remove the barriers that keep EAP utilization chronically low.
Acuity-appropriate matching. Validated screening tools at intake, specifically PHQ-9 for depression and GAD-7 for anxiety, enable matching members to the appropriate level of support. A member with mild subthreshold symptoms is routed to structured self-guided content. A member with moderate depression receives coaching with clinical oversight. A member with severe symptoms or safety concerns is escalated to a licensed clinician or crisis resource. That matching does not happen in an EAP.
Longitudinal clinical outcomes tracking. Programs that administer PHQ-9 and GAD-7 at defined intervals over a member's engagement period can document symptom trajectory, measure meaningful improvement, and connect behavioral health outcomes to chronic condition management programs. That is the measurement infrastructure that makes behavioral health clinically credible and financially accountable in a way that EAP utilization reports cannot achieve.
How EAP and digital behavioral health work together
The frame shift is not EAP versus digital behavioral health. It is understanding what each component is designed to deliver and building a benefits architecture that deploys both appropriately.
EAPs remain the right resource for acute crisis navigation, immediate counselor access, and short-term situational support. They belong in a complete behavioral health benefits portfolio as the acute response layer.
Digital behavioral health programs are the right resource for the population with persistent, chronic, or comorbid behavioral health needs who will never self-navigate to an EAP, whose needs exceed session caps, and whose outcomes need to be tracked and connected to the rest of their clinical picture. They are the population management layer that EAPs were never designed to be.
Solera Health's network addresses Behavioral Health as an integrated condition area, with digital programs matched to members based on clinical profile, acuity level, and comorbidity burden. The Precision Insights Suite identifies members at behavioral health risk using predictive claims modeling, enabling proactive routing before a crisis occurs. The HALO Platform tracks PHQ and GAD outcomes through the program engagement cycle, connecting behavioral health improvement to chronic condition management across the network.
The question is not whether your EAP is good at what it does. The question is whether what it does is enough for the population you are actually trying to serve.
Solera Health connects benefits leaders and health plan executives to evidence-based digital behavioral health programs, matched to member acuity and clinical profile and measured through validated clinical outcomes.
Explore Other Resources
6/1/2026

The Network Effect: Proving the Value of Curated Digital Health
$1,241 — Total cost of care reduction per member
5/15/2026
Employer Health Care Costs in 2026: What’s Driving the Spike and What’s Actually Working
Do Digital Health Programs Reduce Employer Health Care Costs?
4/6/2026
Death By a Thousand Vendors: A Study of 106 Senior Benefits Leaders
More vendors. More spend. More headcount. And yet — the problem is getting worse.
.png)