


1/1/2026
From Elevated to Stage 2: Why Early Intervention Changes the Cost Trajectory
Nearly half of American adults meet the clinical definition of high blood pressure. Most of them are not managing it effectively. And for benefits leaders and health plan executives, the financial consequence of that gap depends almost entirely on when intervention begins.
Hypertension does not announce itself. It accumulates quietly across years, advancing through clinical stages while members remain asymptomatic and largely unaware of the cost trajectory building in their claims data. By the time a member reaches Stage 2, the intervention options have narrowed considerably. Medication is required. The window for lifestyle modification as a standalone strategy has closed. And the downstream risk for stroke, cardiac events, and kidney disease, all of which carry catastrophic claim costs, has grown substantially.
The ROI case for digital hypertension programs is not primarily about treating Stage 2 members. It is about not letting Elevated and Stage 1 members become Stage 2 members in the first place.
The three-stage BP spectrum and what it costs to intervene at each
Under current ACC/AHA guidelines, hypertension is defined across three actionable stages, each with distinct clinical management requirements and materially different cost implications for payers.
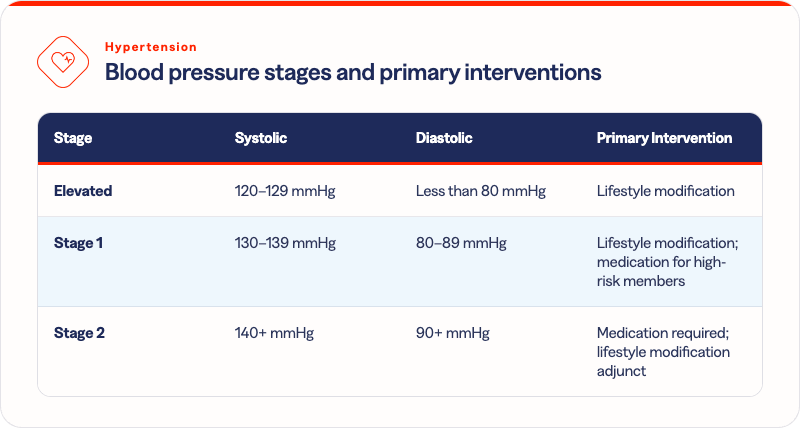
The cost differential between stages is not marginal. Managing a member at the Elevated stage costs a fraction of what Stage 2 management requires, because lifestyle modification, the primary intervention at Elevated and Stage 1, does not carry the medication spend, monitoring intensity, or complication risk that define Stage 2 care.
The average annual medication cost for a member on antihypertensive therapy runs $300 to $900 per year for the drugs alone, before accounting for the physician visits, lab monitoring, and titration appointments that come with ongoing pharmacological management. For members who require multiple agents, which is common at Stage 2, that figure compounds. And none of it addresses the downstream cardiovascular and renal risk that untreated or undertreated hypertension continues to build.
A member who achieves blood pressure normalization through lifestyle modification at the Elevated stage does not enter that cost chain at all. That is the financial case for early intervention, stated plainly.
Why most hypertension programs are designed for the wrong population
Traditional hypertension benefits, including most disease management programs offered by health plans and large employers, are designed around the Stage 2 population. That population is clinically visible in claims data. They are already on medication. They have provider relationships. They generate the utilization that makes them easy to identify and justify targeting.
The problem is that Stage 2 is the most expensive point at which to intervene. The lifestyle modification window has closed. The medication regimen has started. The downstream risk accumulation is already underway. Managing a Stage 2 member well is valuable, but it is damage control rather than prevention.
The Elevated and Stage 1 population is where the cost trajectory is still recoverable. These members have not yet crossed the threshold requiring medication for most presentations. Structured digital support, combining behavioral coaching, nutritional guidance, physical activity programming, and connected device monitoring, can produce clinically meaningful blood pressure reduction without pharmaceutical intervention. For a health plan or self-insured employer, that means a member who does not start a medication regimen, does not escalate to Stage 2, and does not generate the downstream cardiovascular claims that follow uncontrolled hypertension.
And yet this population is systematically underserved. Benefits designs that require a Stage 2 diagnosis for program eligibility exclude exactly the members with the most to gain from early intervention.
What digital programs deliver at the population level
Across Solera's hypertension network, digital programs serving the full BP spectrum, Elevated through Stage 2, document 63 to 71% blood pressure reduction rates among enrolled participants. That outcome range reflects programs combining connected device monitoring, human coaching, and structured behavioral support -- not self-reported estimates.
The clinical significance of those outcomes is direct. A member who moves from Stage 1 to normal range has materially reduced their stroke risk, their cardiac event risk, and their long-term kidney disease trajectory. A member who stabilizes at Elevated rather than advancing to Stage 1 or Stage 2 stays out of the medication cost chain entirely.

The cost of a digital hypertension program is orders of magnitude below the cost of a single preventable cardiac hospitalization. The actuarial case for early intervention is not complicated. The execution gap is structural: most benefits designs do not extend eligibility to the population where early intervention delivers its highest return.
What benefits architecture supports early intervention
Closing the gap between Elevated identification and intervention requires three things most benefits designs do not currently deliver:
- Eligibility that begins at Elevated, not Stage 2. If program access requires a Stage 2 diagnosis, the early intervention window is already closed for the members who enter. Expanding eligibility to include the Elevated and Stage 1 population is the single highest-leverage change a benefits leader can make in hypertension strategy.
- Risk identification before the member self-refers. Members at Elevated and Stage 1 are often asymptomatic and not actively seeking support. Predictive claims analysis that surfaces this population and routes them to programs proactively is how early intervention reaches the members who need it before they advance to higher stages.
- Outcome measurement tied to blood pressure reduction, not engagement. A program that reports enrollment and session completion but cannot document verified blood pressure change is not demonstrating clinical value. Measurement frameworks that require non-self-reported readings and track stage-level progression over time are the standard that separates genuine cost management from wellness participation metrics.
Solera's Precision Insights Suite identifies members across the BP spectrum using predictive claims modeling, routing them to matched programs within the network before Stage 2 is reached. The HALO Platform tracks outcomes through medical claims, connecting blood pressure reduction to the downstream cost avoidance that justifies the investment.
The highest-ROI hypertension investment is not treating Stage 2. It is preventing it.
Solera Health connects benefits leaders and health plan executives to evidence-based digital hypertension programs serving the full BP spectrum, from Elevated through Stage 2, matched to member risk profiles and measured through verified blood pressure outcomes.
Explore Other Resources
6/1/2026

The Network Effect: Proving the Value of Curated Digital Health
$1,241 — Total cost of care reduction per member
5/15/2026
Employer Health Care Costs in 2026: What’s Driving the Spike and What’s Actually Working
Do Digital Health Programs Reduce Employer Health Care Costs?
4/6/2026
Death By a Thousand Vendors: A Study of 106 Senior Benefits Leaders
More vendors. More spend. More headcount. And yet — the problem is getting worse.
.png)