


1/1/2026
The 96 Million Members No One Is Talking To: A Case for Digital Diabetes Prevention
Ninety-six million Americans are living with prediabetes. Eighty percent of them do not know it. They are in your population right now, generating moderate utilization, carrying no diabetes diagnosis, and moving steadily toward one of the most expensive and most preventable chronic conditions in your claims portfolio.
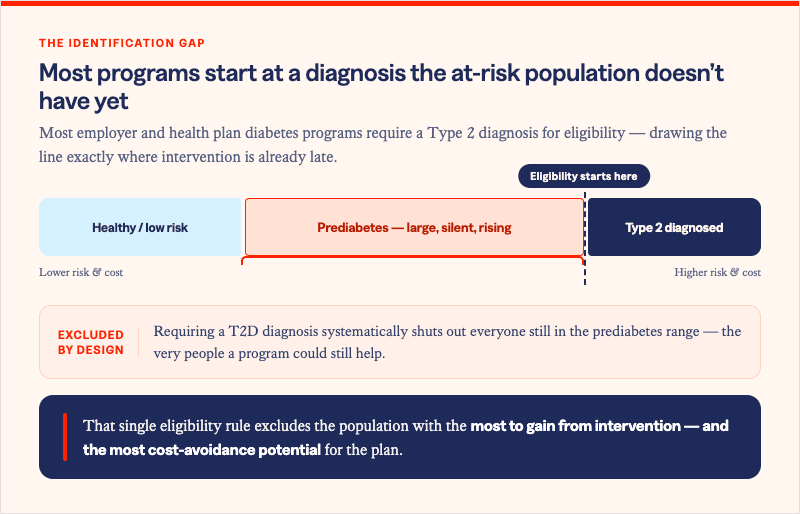
Most diabetes benefits strategy is organized around the members who already have a T2D diagnosis. Disease management programs, medication adherence support, A1C monitoring, endocrinology referrals. That investment is necessary. It is also, from a cost management perspective, the most expensive point at which to intervene.
The members generating tomorrow's diabetes spend are not on your diabetes claims list today. They are on no list at all. And the window to intercept them, before insulin resistance advances to a T2D diagnosis and a lifetime of chronic disease management costs, is finite and closing.
The prediabetes population is large, silent, and expensive in slow motion
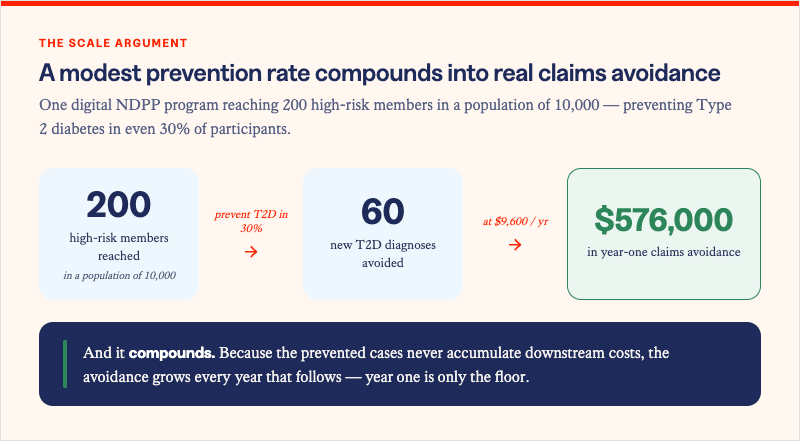
Prediabetes is defined by A1C between 5.7 and 6.4%, or fasting glucose between 100 and 125 mg/dL. It is not a borderline condition. It is a clinical state with documented metabolic progression, and without intervention, approximately 15 to 30% of adults with prediabetes develop type 2 diabetes within five years.
In a self-insured population of 10,000 covered lives, conservative estimates place the prediabetic population at 1,000 to 1,500 members. The vast majority carry no diabetes diagnosis, generate no diabetes-specific claims, and appear nowhere in a standard high-risk member identification pull. They are not invisible because they are healthy. They are invisible because the benefits architecture was not designed to find them.
Their cost trajectory, however, is already building. Members with prediabetes carry elevated cardiovascular risk, higher rates of hypertension, and greater MSK-related utilization than normoglycemic peers -- all before a T2D diagnosis appears in their record. The claims they are generating today are not labeled diabetes. They will be.
The intervention window and what it is worth
The evidence for prediabetes intervention is among the strongest in all of preventive medicine. The Diabetes Prevention Program Outcomes Study, published in the New England Journal of Medicine, found that lifestyle intervention producing 5-7% body weight loss reduced T2D onset by 58% in high-risk adults. That figure has been replicated across populations, health systems, and delivery models for more than two decades.
For comparison: metformin, the standard pharmacological intervention for high-risk prediabetic adults, achieved a 31% risk reduction in the same study. The lifestyle intervention outperformed the drug on the primary outcome. And unlike metformin, the behavioral intervention does not require ongoing prescription costs, does not carry adherence burden as a primary failure mode, and produces benefits across multiple conditions simultaneously.
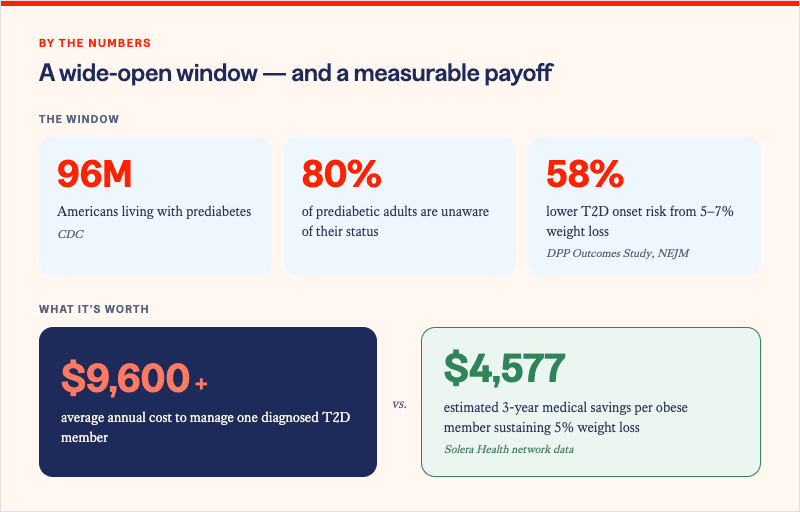
The financial translation is direct. A member who does not develop type 2 diabetes does not enter a lifetime of chronic disease management spend. The average annual cost of managing a T2D member exceeds $9,600, before accounting for the downstream cardiovascular, MSK, and behavioral health costs that co-occur at elevated rates in this population. Preventing a single case of T2D in a high-risk member represents a multi-year, compounding claims avoidance that dwarfs the cost of the intervention that produced it.
Why digital delivery changes the scale equation
The clinical evidence for diabetes prevention has existed for more than two decades. The gap is not the evidence. It is delivery infrastructure. Traditional diabetes prevention programs required in-person group sessions, limiting geographic reach, participant availability, and program scale. For large employers and health plans managing populations across multiple states, that model was never viable at scale.
CDC-recognized digital NDPP programs solve the delivery problem without compromising the clinical evidence base. They replicate the behavioral coaching, nutritional guidance, and accountability structure of the original DPP in a format members can access from anywhere, at any time, through any device. The CDC's recognition framework requires that digital programs meet the same outcome standards as in-person models: documented participant weight loss and session completion at defined thresholds.
For health plans and self-insured employers, digital delivery also solves the billing problem. CDC-recognized NDPP programs bill through medical claims under established coding, making them reimbursable under most commercial plan designs. Under the ACA, NDPP is a covered preventive service without cost-sharing for eligible participants. That benefit design removes the access friction that makes most wellness programs underperform: no out-of-pocket cost, no referral required, no in-person visit to schedule.
Finding the population before the diagnosis finds them
The practical barrier to diabetes prevention at scale is not program availability. It is identification. Members do not self-refer to diabetes prevention programs. They are not searching for them. They frequently do not know they are at risk.
Reaching the prediabetic population requires proactive risk identification through claims data analysis, not passive enrollment. Predictive modeling that surfaces members with A1C values in the prediabetic range, BMI above 25 with metabolic risk factors, or utilization patterns consistent with insulin resistance can identify intervention candidates months or years before a T2D diagnosis appears in their record.
Solera's Precision Insights Suite also applies proprietary predictive AI across your own claims data to identify members who will be cost bloomers before they start incurring high investment treatments. Through varied interventions, those members can be routed either to CDC-recognized digital NDPP programs within the network, matched to their clinical profile and risk level, or to other care in your network. The result is proactive outreach to a population that would otherwise remain invisible until their prediabetes becomes diabetes.
The members who will generate your highest diabetes spend over the next five years are in your population today. Most of them are not on any program. Most of them do not know they need to be. The benefits architecture that finds them now, before the diagnosis, is the one that bends the curve.
Explore Other Resources
6/1/2026

The Network Effect: Proving the Value of Curated Digital Health
$1,241 — Total cost of care reduction per member
5/15/2026
Employer Health Care Costs in 2026: What’s Driving the Spike and What’s Actually Working
Do Digital Health Programs Reduce Employer Health Care Costs?
4/6/2026
Death By a Thousand Vendors: A Study of 106 Senior Benefits Leaders
More vendors. More spend. More headcount. And yet — the problem is getting worse.
.png)