


1/1/2026
The GLP-1 Question Every Benefits Leader Is Actually Asking
Every benefits leader is asking some version of the same question about GLP-1 medications: should we cover them, how do we manage the cost, and what happens when members stop taking them? The first question is largely settled. The second is where most strategies stall. The third is the one that will determine whether your GLP-1 investment produces durable value or a recurring cost problem.
GLP-1 receptor agonists are clinically effective for weight loss. The evidence is not in dispute. Trials document meaningful average weight reductions in members who take these medications consistently, with associated improvements in glycemic control, blood pressure, and cardiovascular risk markers. For members with obesity and related comorbidities, they represent a genuine clinical advance.
The benefits strategy question is not whether GLP-1 medications work. It is whether a medication-only approach, without the behavioral change infrastructure that makes weight loss durable, is a cost management strategy or a cost deferral strategy. That distinction is worth getting right before your formulary decision is made.
The discontinuation problem no one is planning for
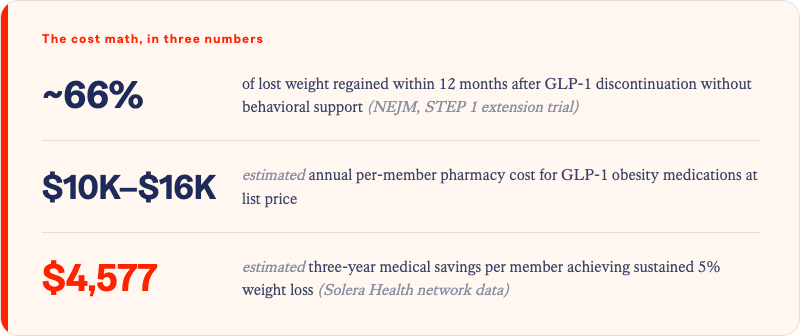
Clinical trial data on GLP-1 discontinuation is unambiguous: members who stop taking these medications without established behavioral change infrastructure regain the majority of lost weight within 12 months. One widely cited trial found that participants who discontinued the medication after achieving significant weight loss regained approximately two-thirds of that weight within a year. The physiological mechanisms that drive weight regain do not pause because a member achieved results on medication.
For a self-insured employer or health plan, that trajectory has a direct cost consequence. A member who loses 15% of body weight on a GLP-1 medication, accrues the associated pharmacy spend, and then discontinues and regains most of that weight has not generated a durable health outcome. They have generated a temporary clinical result at a permanent cost.
The discontinuation rate for GLP-1 medications in real-world commercial populations is substantially higher than in clinical trials. Reasons vary: side effect burden, cost after coverage changes, access gaps, and loss of motivation once initial results plateau. In practice, a meaningful percentage of members who start GLP-1 therapy will not sustain it. Planning for that reality is not pessimism. It is actuarial responsibility.
The cost math of medication without support
GLP-1 medications for obesity carry annual pharmacy costs that typically range from $10,000 to $16,000 per member at list price before rebates and plan negotiation. Even at significantly discounted net costs, they represent a substantial per-member investment. Benefits leaders evaluating coverage decisions need to model not just the cost of coverage but the cost of the outcomes that coverage produces, and fails to produce, over a three-to-five year horizon.
The math that most GLP-1 coverage analyses do not include is the cost of the rebound cycle: a member who loses and regains weight repeatedly does not return to their pre-treatment cost baseline. They may return to their pre-treatment weight while having accumulated pharmacy spend, experienced metabolic fluctuation, and potentially developed new comorbid conditions in the process. The question is not just what GLP-1 coverage costs. It is what GLP-1 coverage without behavioral support infrastructure produces over time.
What makes a GLP-1 strategy durable
The evidence base for combining GLP-1 therapy with behavioral support is materially stronger than medication alone on long-term weight maintenance. Members who pair pharmacotherapy with structured behavioral programming, medical nutrition therapy, and ongoing clinical engagement show better weight maintenance at 12 and 24 months than those receiving medication without that infrastructure.
- Behavioral change programs. Structured digital weight management programs that incorporate evidence-based behavioral coaching, habit formation protocols, and accountability frameworks address the lifestyle dimension that medication cannot. Members who develop sustainable eating and activity patterns while on GLP-1 therapy are better positioned to maintain outcomes if and when medication is discontinued.
- Medical nutrition therapy. Registered dietitian support tailored to a member's metabolic profile, comorbidities, and medication regimen directly addresses the dietary component of long-term weight maintenance. Medical nutrition therapy is reimbursable under many commercial benefit designs and generates measurable outcomes in glycemic control, lipid management, and sustained weight maintenance, outcomes that compound over time for members on GLP-1 therapy.
- Virtual clinical care. Ongoing clinical oversight that monitors metabolic markers, adjusts support intensity as a member's needs change, and bridges the gap between primary care visits sustains engagement through the phases where dropout risk is highest. Virtual clinical care extends the reach of the clinical relationship without requiring in-person visit frequency that most members cannot sustain.
Together, these three components constitute the infrastructure that converts a medication outcome into a durable health outcome. Without them, GLP-1 coverage is a pharmacy benefit. With them, it becomes a weight management strategy with a defensible long-term ROI.
How Solera's network supports a durable GLP-1 strategy
Solera Health's network includes evidence-based digital weight management programs, medical nutrition therapy, and virtual clinical care matched to member risk profiles through the HALO Platform. Members on GLP-1 therapy can be routed to behavioral and clinical support programs that reinforce medication outcomes, address the lifestyle dimensions that medication does not, and provide the ongoing engagement structure that reduces discontinuation risk.
The clinical case for GLP-1 medications is settled. The benefits strategy case depends entirely on what surrounds them.
Solera Health connects benefits leaders and health plan executives to evidence-based digital weight management programs, medical nutrition therapy, and virtual clinical care, matched to member risk profiles and measured through medical claims outcomes.
Explore Other Resources
6/1/2026

The Network Effect: Proving the Value of Curated Digital Health
$1,241 — Total cost of care reduction per member
5/15/2026
Employer Health Care Costs in 2026: What’s Driving the Spike and What’s Actually Working
Do Digital Health Programs Reduce Employer Health Care Costs?
4/6/2026
Death By a Thousand Vendors: A Study of 106 Senior Benefits Leaders
More vendors. More spend. More headcount. And yet — the problem is getting worse.
.png)