


1/1/2026
Why Behavioral Health Is the Missing Piece in Your Weight Management Strategy
Most weight management programs are designed as if the only barrier to weight loss is information. Eat differently. Move more. Follow the plan. That framing misses the clinical reality for a substantial share of the members enrolled in those programs, and it is a primary reason why program completion rates and sustained outcomes fall well below what the evidence base for weight management actually promises.
The missing variable is behavioral health. Not as a separate benefit. Not as a referral pathway bolted onto a weight management program. As an integrated component of the clinical model from day one.
For benefits leaders evaluating weight management programs or trying to understand why their current investment is not producing the outcomes the vendor's case studies suggest it should, the behavioral health connection is where the answer almost always lives.
Depression and obesity are not separate problems
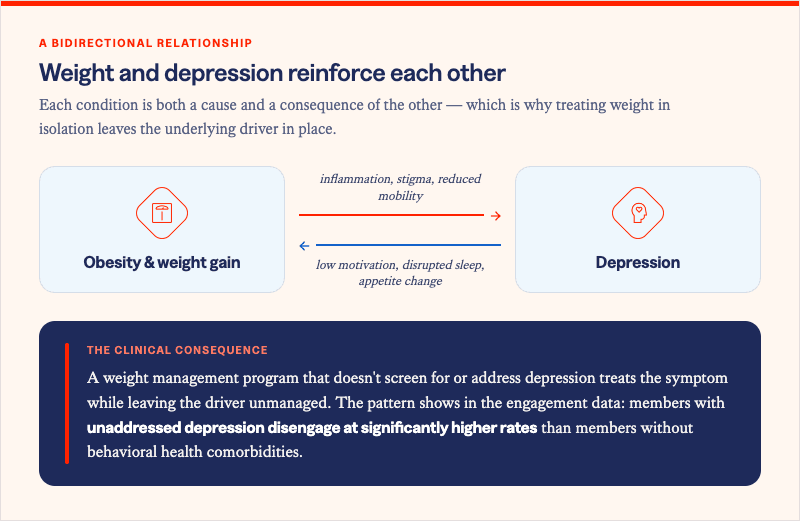
The relationship between depression and obesity is bidirectional, clinically documented, and operationally underaddressed in most employer benefits portfolios. Adults with obesity are 55% more likely to develop depression over time. Adults with depression are 58% more likely to develop obesity. These are not correlations. They are reinforcing clinical pathways that run in both directions simultaneously.
Depression drives weight gain through multiple mechanisms. Reduced motivation impairs physical activity. Disrupted sleep alters metabolic hormones, specifically leptin and ghrelin, in ways that increase appetite and reduce satiety signaling. Emotional eating as a coping strategy is not a behavioral quirk -- it is a neurologically mediated response to chronic stress and low mood. And the fatigue associated with depression makes the energy required to sustain a structured weight management program feel categorically different than it does for members who are not carrying that burden.
Obesity, in turn, physiologically worsens depression. Adipose tissue, particularly visceral fat, produces inflammatory cytokines that cross the blood-brain barrier and directly affect neurotransmitter function. Insulin resistance, which accompanies obesity in many members, is independently associated with depressive symptoms. Social stigma and reduced physical function compound the psychological burden. A member who enters a weight management program while carrying untreated depression is not simply less motivated. They are managing a clinical condition that is actively working against every behavioral change the program is asking them to make.
What unaddressed behavioral health does to program performance
The impact of untreated depression and anxiety on weight management program completion is measurable and substantial. Research consistently shows that members with active depression enrolled in standard behavioral weight loss programs complete fewer sessions, achieve lower average weight loss, and are significantly more likely to regain weight in the 12 months following program completion than members without depression.
For benefits leaders, that completion data has a direct financial implication. A weight management program with a 40% completion rate among members with unaddressed behavioral health comorbidities is not delivering the ROI its outcomes data promises -- because that outcomes data was almost certainly generated in a population with higher behavioral health stability than your enrolled members.
The engagement gap also compounds over time. A member who disengages from a weight management program early does not simply fail to lose weight. They often experience increased demoralization about future program participation, making re-enrollment less likely and increasing the probability that the underlying metabolic risk continues to accumulate untouched.
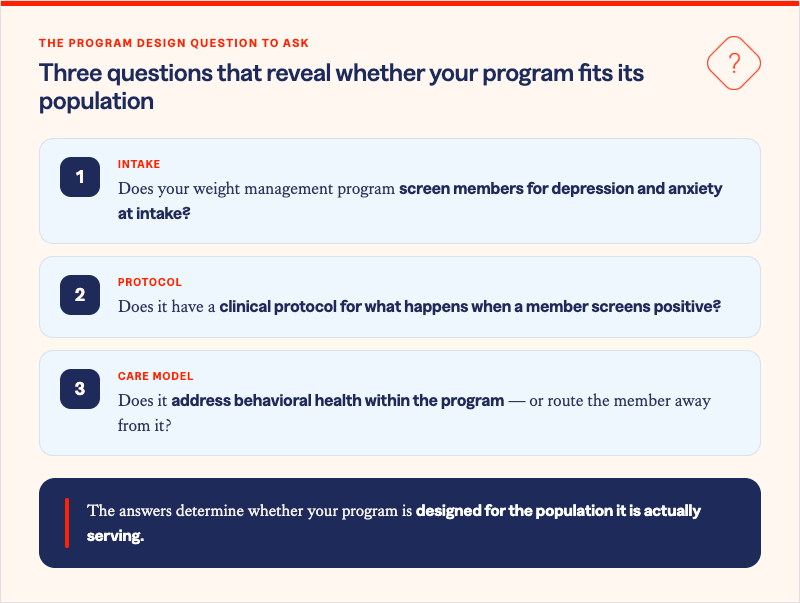
This is not a member motivation problem. It is a program design problem. A weight management model that treats behavioral health as a separate referral rather than an integrated clinical component is structurally unlikely to retain the members who most need it.
Why integrated programs outperform siloed ones
The evidence for integrated weight management and behavioral health support is consistent across study designs. Members who receive simultaneous support for weight loss and depression or anxiety -- within the same program, from a coordinated clinical team, with shared outcome measurement -- show materially better results on both dimensions than members receiving either intervention alone.
The mechanism is straightforward. When a member's depressive symptoms are improving, their capacity to engage with behavioral change increases. When their weight is declining, the physiological drivers of depression, including inflammatory burden and insulin resistance, are also improving. These are not parallel processes. They are mutually reinforcing ones, and a program designed to activate both simultaneously captures the clinical benefit of that reinforcement rather than working against it.
Integration also removes the friction of separate engagement channels. A member managing depression and excess weight who must navigate two separate programs, two separate portals, two separate care teams, and two separate check-in cadences is less likely to sustain engagement with either than a member whose clinical support is unified. Every additional navigation step is an attrition risk, and members with active depression are particularly sensitive to friction.
What Solera's integrated model delivers
Solera Health's network addresses Weight Management and Behavioral Health as connected condition areas, with evidence-based digital programs matched to members based on their full clinical profile, not just their primary diagnosis. For members presenting with both excess weight and behavioral health risk, that means access to integrated support that addresses both dimensions simultaneously, within a coordinated network measured through medical claims outcomes. The Solera HALO Platform connects those members to programs designed for clinical complexity, not just the median enrolled member.
A weight management benefit that ignores behavioral health is not a cost-neutral oversight. It is a structural gap that reduces program effectiveness for precisely the members whose successful outcomes would generate the most downstream claims savings.
The behavioral health connection is not a soft add-on to weight management strategy. It is the variable that determines whether your program produces the outcomes it is capable of delivering.
Solera Health connects benefits leaders and health plan executives to evidence-based digital health programs spanning Weight Management and Behavioral Health, matched to member clinical profiles and measured through medical claims outcomes.
Explore Other Resources
6/1/2026

The Network Effect: Proving the Value of Curated Digital Health
$1,241 — Total cost of care reduction per member
5/15/2026
Employer Health Care Costs in 2026: What’s Driving the Spike and What’s Actually Working
Do Digital Health Programs Reduce Employer Health Care Costs?
4/6/2026
Death By a Thousand Vendors: A Study of 106 Senior Benefits Leaders
More vendors. More spend. More headcount. And yet — the problem is getting worse.
.png)